
Across the country, racial disparities in birth outcomes reflect a large health inequity — one that means Black women and infants are dying from preventable pregnancy-related complications at higher rates than other demographic groups.
Unfortunately, this trend holds true in Chatham, according to a report on health disparities just released by the Chatham County Public Health Department. It’s a reality the department is partnering with many other local health officials and community members to work toward changing, according to CCPHD Strategic Planning and Development Officer Casey Hilliard.
“Although we are investigating what is contributing to the disparities in infant mortality and low and very low birth weights in our county, we do know that racial disparities in birth outcomes are a well-documented and troubling reality across the country,” Hilliard said. “The evidence, including studies that show that these disparities are persistent across income and education levels, points to racism as a root cause of these unequal outcomes.”
The report is part of the department’s work to pursue health equity in the community; in addition to examining maternity wellness, the report also included rates related to COVID-19, mental health, life expectancy and more. Health disparities, the report said, are the consequence of “structural inequities that push communities into the margins and create the external factors that redirect, reduce, and remove opportunities to achieve optimal health.”
Hilliard emphasized that it’s the combination of structural racism — “which contributes to poorer quality of care and unequal access to care and the social drivers of health” — along with the experience of racism over a person’s lifetime, which drives inequities in birth outcomes.
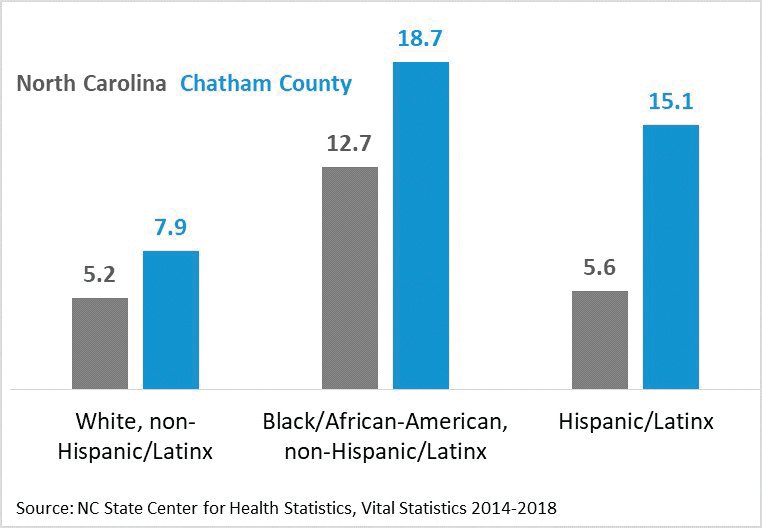
In Chatham County, infant mortality rates are higher among both Black and Hispanic residents than white residents — 18.7 and 15.1 per 1,000 live births, compared with 7.9.
“It is worth noting that the disparate outcomes for Hispanic/Latinx women and babies in Chatham County are not mirrored in state and national statistics,” Hilliard said. Nationally, racial and ethnic disparities in pregnancy-related dealths affect Black, American Indian/Alaskan Native women at the highest rates, according to a 2019 report from the Centers for Disease Control and Prevention.
“We are not sure why birth outcomes are worse for Hispanic/Latinx women in Chatham,” Hilliard said, “but we are concerned and committed to addressing these inequities through collective system-level solutions.”
One large part of such solutions is the new Chatham Hospital Maternity Care Center, which became the first maternity center in the county in nearly 30 years when it opened in September. Prior to the maternity center opening, Hilliard said, Chatham ranked in the bottom quarter of North Carolina counties for average distance between a resident’s home and a hospital offering childbirth services — 25 miles and upwards of 30 to 40 minutes.
“Bringing quality maternity care to this critical access rural hospital will have a ripple effect for the health of women and babies in Chatham. In fact, it already has,” she said.
Chatham Hospital Chief Medical Officer Dr. Andy Hannapel echoed this sentiment, stating it’s important to have a safe place within the community where maternity needs are met.
“Chatham County and surroundings are subject to these same trends and have contributing factors similar to other U.S. and N.C. communities — especially around rural health care issues of access and limited resources,” he said.
Hannapel highlighted another big part of the community’s efforts to address disparate maternal and infant outcomes in Chatham: Equity for Moms and Babies Realized Across Chatham (EMBRACe). A two-year grant-funded project aimed at achieving equitable birth outcomes in the county, EMBRACe is a product of collaboration between Chatham Hospital, CCPHD, Piedmont Health Services, Chatham County Department of Social Services and Chatham Health Alliance.
“Chatham Hospital, together with our community partners, wants to create and maintain a welcome, safe place for people to come and receive the care that they need and that they seek,” Hannapel said. “It isn’t enough that we spent $2.6 million to build the Maternity Care Center. We have to make this a part of the safe community space with PHS, CCPHD, CCDSS — where mothers and their babies come for care.”
Through partnerships to share leadership, decision-making and data, the project specifically focuses on advancing policies, practices and programs “to ensure all women receiving prenatal and perinatal care are treated with dignity and respect,” Hilliard said.
Ellen Chetwynd, a lactation consultant and researcher who’s led maternal health efforts at UNC Family medicine, is one of the founding member of EMBRACe. She said she was initially drawn to the project because of the aligned vision to bring maternity care to an area that was previously a “maternity care desert.”
“It just was such a beautiful fit to have two years to really focus on systems and alignment of services and integration of care, which, you know, even though everybody wanted it, nobody really had the time to focus on that specifically,” she said.
Chetwynd was also inspired by a doula program she encountered in Asheville, SistersCaring4Sisters — founded by women of color for women of color.
“That was one of the stories that fed into EMBRACe, just this example of another group of people who had come together around a topic area and created something that was truly based on community desires,” she said.
Chetwynd has helped lead the community engagement piece of the project, with experience holding listening sessions in English and Spanish to hear from women in Chatham what they were looking for in Chatham’s maternity care center.
EMBRACe hosted one listening session before COVID-19 hit, Chetwynd said, meaning their engagement efforts were temporarily postponed. Now, the group will be hosting sessions online, focusing on more of a “storytelling format” than a formal focus group one.
“It’s tough to run a maternity care unit in a rural setting — they’re expensive,” Chetwynd said, referencing the hospital’s efforts to connect with other rural maternity centers prior to opening. “We’ve been at this now since January, we’re nine months in and I think we’ve got a good solid base. That’s not very interesting, but literally within the last couple of weeks we’ve started to take the first steps toward launching into our actual efforts. I think we’ve done some solid work.”
Along with the logistical challenges COVID-19 has brought for the project, it’s also exposed the many inequalities in health care delivery and access, Hannapel said. He added that work done to address these disparities must not focus on the outcomes that result from the system such as exposure, illness, or death but the root case — “a system that discriminates on the basis of economic status (the poor, the uninsured), race and ethnicity.”
“This is difficult for all of us because that is not how we see ourselves in America as Americans. But the truth is — this is the system we have and participate in,” Hannapel said. “EMBRACe has developed a structure to examine this in each of the community entities and provide this information back to the individual institution and the group. We want to be informed and coordinated across the community partners in our policies and practices. This work towards consistency across entities... I believe, will help our patients.”
Reporter Hannah McClellan can be reached at hannah@chathamnr.com.